
EDITORIAL
Andrés F. Cardona¹, Christian Rolfo², Umberto Malapelle³, Diego de Miguel-Pérez²
Institute of Research, Science and Education, Luis Carlos Sarmiento Angulo Cancer Treatment and Research Center – CTIC, Bogotá, Colombia
Center for Thoracic Oncology, The Tisch Cancer Institute, Mount Sinai Health System and Icahn School of Medicine, New York, NY, United States
Medical Oncology Unit A.O. Papardo & Department of Human Pathology, University of Messina, Italy
Recibido:
1 de noviembre, 2023
Aceptado:
15 de noviembre, 2023
Correspondencia:
DOI: 10.56050/01205498.2306
The use of liquid biopsy (LB) has become highly relevant in the clinical field, and the acquisition of circulating free DNA (cfDNA) has become consolidated as an emerging biomarker and a tool for the research, diagnosis, and prognosis of solid tumors (1). Different studies have confirmed that this type of DNA contains information on specific tumor-related alterations, such as mutations, methylations, and copy number variants (CNVs) (2). The most striking advantage of LB is its ability to isolate ctDNA through a minimally invasive technique (1,3).
ctDNA is released into the bloodstream due to cellular processes such as apoptosis, pyroptosis, mitotic catastrophe, autophagy, phagocytosis, or NE- Tosis (4). In patients with cancer, the levels of ctDNA are higher, and thus, the structural and epigenetic changes in the DNA sequence can be observed and reflect the disease process (5,6). Also, LB provides real-time information about the tumor, which is relevant because it is temporary and spatially heterogeneous. The detection of these variations positively impacts timely treatment modifications that could be beneficial for the patient (7,6). Notably, analyzing nucleic acids in tumor tissue from traditional biopsies provides predominant tumor cells. In contrast, the tumor analysis through cfDNA is derived from all tumor sites. This allows LB to monitor a patient’s disease burden more accurately and progression in real-time, thus detecting information about the heterogeneity of different tumors (8).
Another significant advantage is that the cfDNA released by the tumor into the bloodstream has the same variants as those of the tumor cells. This allows us to have information at different times of the disease, and given the ease of sampling, repeated sampling is possible without further inconvenience to the patient (8). This knowledge has led to significant technological advances, including the isolation of cancer cells and the collection of DNA derived from them, to have accurate and timely information through LB of oncogene-related variants taken into account for the design of targeted therapies (9). In this context, the LB is a powerful resource to determine the appearance of additional genetic changes, such as the drug resistance mutations that appear with specific targeted therapies. In this way, the possibility of taking repeated samples allows adjusting the therapy to respond to the evolution of the tumor (6). Likewise, it is also possible to obtain ctDNA in several body fluids such as urine, feces, cerebrospinal fluid, and saliva (8,9). Thus, advances in this field will undoubtedly change how the treatment of a patient with cancer is selected and monitored.
The development of precision medicine (PM) represented a breakthrough in cancer management (1,7). The application of individualized treatments emphasizing tumor biology and predictive responses has significantly improved clinical outcomes. Hence, the clinical applications of PM are broad, encompassing screening, diagnosis, prognosis, prediction of treatment response and resistance, early detection of recurrence/metastasis, and biological cancer stratification (2). However, challenges related to early diagnosis and real-time treatment monitoring remain. Some of these issues are due to previously described tumor biopsies, including limited tissue availability, the continuously evolving tumor genetic landscape in response to treatment, the emergence of resistant subclones, and the need for knowledge on spatial and temporal heterogeneity of tumoral cells (3). Figure 1 includes the major developments in the history of liquid biopsy for cancer diagnosis and monitoring.
The completion of the Human Genome Project (HGP) in 2001 opened the floodgates to a deeper understanding of the diseases and their potential treatment (10). Therapeutic advances in genome-guided precision oncology rely upon the prospective molecular identification of oncogenic alterations and resistance mechanisms to guide accurate treatments (5). Technological advances in the genetic sequencing of circulating free DNA (cfDNA) in plasma have enabled LB that has the potential to identify actionable alterations in tumor-derived DNA present in blood and other fluids and capture intra-tumoral heterogeneity not addressed by tumor tissue biopsy (that only captures a single site), potentially avoiding the need for invasive measures that consume time and generate unnecessary risks. Following the same perspective, ctDNA is often present in patients without detectable circulating tumor cells, suggesting that these two biomarkers represent distinct entities. As failure rates at large academic cancer centers from diagnostic tests derived from tissue biopsy-based next-generation sequencing (NGS) are approximately 14%, ctDNA analysis may be helpful in guiding treatment selection in patients for whom tissue-based NGS is not an option (6).
LB has been recently gaining attention as an alternative to traditional tissue biopsies, given their minimally invasive nature providing a vast amount of information (5). The most commonly used techniques are quantification of ctDNA and circulating tumor cells (CTCs) (5,6). Detection of specific genetic abnormalities based on mutation identification and DNA methylation analyses, both genome-wide and site-specific, have also been gaining relevance (7). Furthermore, ctDNA carries some genomic and epigenomic alterations concordant to the tumor mutational spectrum, such as point mutations, degree of integrity, rearranged genomic sequences, copy number variation (CNV), microsatellite instability (MSI), loss of heterozygosity (LOH), and DNA methylation (8). These biological characteristics discriminate ctDNA from normal cfDNA and reinforce the latter as a specific biomarker that provides personalized information to detect residual disease or monitor tumor progression during therapy (9).
Figure 1. Major advances in the history of liquid biopsy for cancer screening, diagnosis, and monitoring.
Under normal circumstances, in healthy individuals, apoptotic and necrotic cells are cleared up by infiltrating phagocytes, and cfDNA levels are relatively low. However, this mechanism does not act effectively with tumoral masses. In solid tumors, ctDNA can also be released through necrosis, autophagy, and other physiological events induced by microenvironmental stress and treatment pressure(6). The size of most fragments ranges between 180 and 200 base pairs (bp), suggesting apoptosis as the predominant source of ctDNA (9). Figure 2. includes the main differential characteristics, indications, and opportunities of LB in solid and hematological tumors.
Advances in LB as prognostic and predictive tools are primarily associated with lung, colon, and breast cancer (BC). Interestingly, each histology has been preferably associated with a particular type of LB. While research in lung or colon cancer has been linked to ctDNA analyses, for BC, the combination of ctDNA and CTCs is more widely used (8). Advancements have been mainly achieved in the metastatic setting, as the amount of CTCs and ctDNA, which increase with tumoral burden, is the greatest.
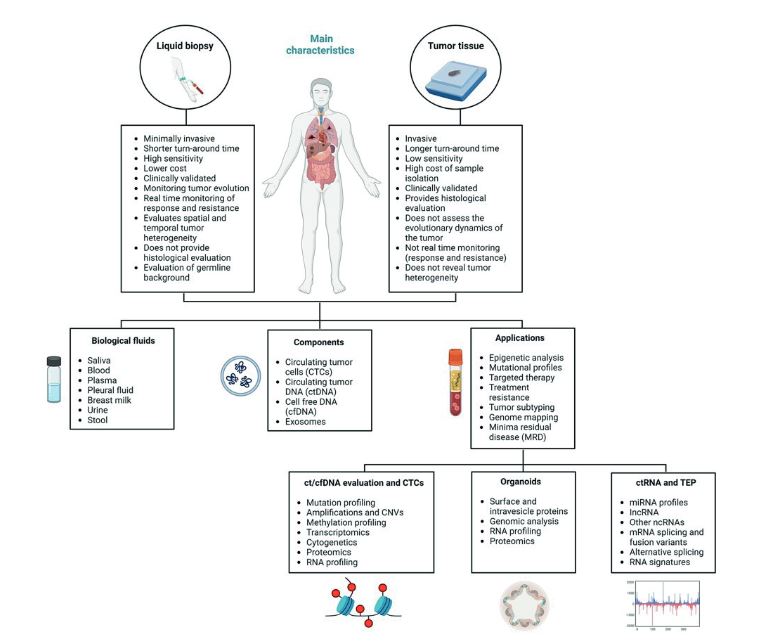
Figure 2. Main differential characteristics, indications, and opportunities of LB in cancer.
This, in turn, offers the best disease model for monitoring and assigning new therapies (3). Particularly in the case of lung cancer, many multidisciplinary efforts have been made to advance the clinical application of LB. In this regard, standardized isolation methods, such as solid-phase extraction techniques, have been used to isolate ctDNA, and many sequencing or mutationanalysis methods have been developed to study and understand their clinical implication (11). Furthermore, with the current development of high-throughput techniques for NGS, the evaluation of gene panels is expected to be included as routine analysis, especially for the screening of high-risk individuals. Concerning treatment management, ctDNA has been used in non-small cell lung carcinoma (NSCLC) for targeted therapy selection, treatment monitoring, and detectionof resistance mechanisms using the identification of somatic mutations in the EGFR gene. The Cobas® EGFRMutation Test v2 (Roche) was the first LB test approved by the US-FDA in June 2016 for the detection of EGFR exon 19 deletions or exon 21 (L858R) substitution mutations in NSCLC patients (12). This represented significant progress in the clinical utility of cDNAs.
In the case of colorectal cancer (CRC), detection of ctDNA in plasma has been associated with worse survival outcomes compared to undetectable levels (5). Additionally, a strong association between ctDNA positivity and recurrence-free survival (RFS) and overall survival (OS) in patients with CRC, irrespective of tumor stage, study size, tumor markers, detection methods, and sample type, is also worth noticing (5,13). The utility of ctDNA as a prognostic parameter and alternative modality for mutation detection before treatment in metastatic CRC (mCRC) was demonstrated in the randomized CORRECT phase III trial. The progression-free survival (PFS) of patients with KRAS mutations detected in plasma treated with regorafenib was shorter than those without mutations (14). Therefore, the prognostic value of KRAS mutations in plasma without requiring tissue confirmation was established (5). This allowed the development of several ctDNA mutation assays and platforms for KRAS mutation screening and treatment selection, such as the IdyllaTM and Cobas®, both FDA-approved. BC was one of the first tumor models in which different types of liquid biopsies were studied. In BC, the prognostic value of ctDNA was documented in numerous studies showing the clinical value of detecting HER2 amplification, PIK3CA, and ESR1 mutations in ctDNA (15).
In recent years, ctDNA analyses have been reviewed in other different neoplasia such as liver, pancreas, ovarian, or prostate cancer (4). In the case of pancreatic cancer (PC), one of the most aggressive and devastating malignancies, the absence of a reliable methodology for early identification and limited therapeutic options for advanced disease offer a possibility for broad LB implementation (16). In this context, a study conducted by Shapiro et al. reported that the presence of ctDNA in PC is markedly elevated compared to healthy controls, concluding that ctDNA may serve as a useful diagnostic and prognostic biomarker (17). Similar studies show that PC patients with noticeable ctDNA experience worse survival and greater risk of diagnosis at an advanced disease stage (18). Tjensvoll et al. also noted that during chemotherapy, changes in mutant KRAS circulation levels corresponded to radiological response assessments and CA19-9 values, suggesting the utility of ctDNA for monitoring treatment efficacy and tumor progression (19). These studies demonstrated the potential clinical utility of ctDNA as a prognostic marker in PC.
In the case of ovarian cancer, previously, there was a lack of reliable screening strategies. However, the clinical value of ctDNA-based assays was demonstrated (3). The first study on LB for screening using copy-number variation (CNV) detection in cfDNA, conducted by Cohen et al., obtained satisfactory results (20). Similar studies are being developed for other solid tumors, including hepatocellular carcinoma, head and neck, and prostate cancer (21,22). However, in other tumor types, ctDNA studies still need to be explored. Current standard clinical tools for diagnosing and monitoring central nervous system (CNS) tumors have several significant limitations (23). Mainly the requirement of invasive tissue sampling with a higher risk of complications relative to other locations and the decreased feasibility of repetitive sampling. Therefore, using LB in patients with CNS malignancies is particularly attractive. However, further studies are still necessary (24).
In conclusion, clinical evidence confirms increased levels of ctDNA, particularly in metastatic disease in patients with any of the solid tumors analyzed so far. Furthermore, ctDNA levels in cancer patients likely correlate with tumor burden, stage, vascularity, cellular turnover, and response to therapy. However, not all metastatic tumors seem to have the same impact on ctDNA levels, and more research is required since critical clinical standards (including uniform pre-analytic and analytical phases) are scarce and need to be established (6). The harmonization of studies and comparative studies is crucial to provide clear evidence of the clinical utility of ctDNA in metastatic solid tumors.
Aarthy R, Mani S, Velusami S, Sundarsingh S, Rajkumar T. Role of Circulating Cell-Free DNA in Cancers. Mol Diagn Ther. 2015;19(6):339-50. doi: 10.1007/ s40291-015-0167-y.
Hiley C, de Bruin EC, McGranahan N, Swanton C. Deciphering intratumor heterogeneity and temporal acquisition of driver events to refine precision medicine. Genome Biol. 2014;15(8):453. doi: 10.1186/ s13059-014-0453-8.
Bettegowda C, Sausen M, Leary RJ, Kinde I, Wang Y, Agrawal N, et al. Detection of circulating tumor DNA in earlyand late-stage human malignancies. Sci Transl Med. 2014;6(224):224ra24. doi: 10.1126/scitranslmed.3007094.
Bronkhorst AJ, Ungerer V, Holdenrieder S. The emerging role of cell-free DNA as a molecular marker for cancer management. Biomol Detect Quantif. 2019;17:100087. doi: 10.1016/j.bdq.2019.100087.
Loft M, To YH, Gibbs P, Tie J. Clinical application of circulating tumour DNA in colorectal cancer. Lancet Gastroenterol Hepatol. 2023;8(9):837-852. doi: 10.1016/S2468-1253(23)00146-2.
Sisodiya S, Kasherwal V, Khan A, Roy B, Goel A, Kumar S, et al. Liquid Biopsies: Emerging role and clinical applications in solid tumours. Transl Oncol. 2023;35:101716. doi: 10.1016/j.tranon.2023.101716.
Mathai RA, Vidya RVS, Reddy BS, Thomas L, Udupa K, Kolesar J, et al. Potential Utility of Liquid Biopsy as a Diagnostic and Prognostic Tool for the Assessment of Solid Tumors: Implications in the Precision Oncology. J Clin Med. 2019;8(3):373. doi: 10.3390/jcm8030373.
Arnedos M, Vicier C, Loi S, Lefebvre C, Michiels S, Bonnefoi H, et al. Precision medicine for metastatic breast cancer--limitations and solutions. Nat Rev Clin Oncol. 2015;12(12):693-704. doi: 10.1038/nrclinonc.2015.123.
Patel KM, Tsui DW. The translational potential of circulating tumour DNA in oncology. Clin Biochem. 2015;48(15):957-61. doi: 10.1016/j.clinbiochem.2015.04.005.
Dweh TJ, Pattnaik S, Sahoo JP. Assessing the impact of meta-genomic tools on current cutting-edge genome engineering and technology. Int J Biochem Mol Biol. 2023;14(4):62-75.
Nigro MC, Marchese PV, Deiana C, Casadio C, Galvani L, Di Federico A, et al. Clinical Utility and Application of Liquid Biopsy Genotyping in Lung Cancer: A Comprehensive Review. Lung Cancer (Auckl). 2023;14:11-25. doi: 10.2147/LCTT.S388047.
The ASCO Post. FDA Approves cobas EGFR Mutation Test v2 as Companion Diagnostic With Gefitinib in First-Line Treatment of NSCLC [Internet]. 2018 [Consultado junio 1 de 2019]. Disponible en: https://www.ascopost.com/News/59214
Basnet S, Zhang Z-Y, Liao W-Q, Li S-H, Li P-S, Ge H-Y. The Prognostic Value of Circulating Cell-Free DNA in Colorectal Cancer: A Meta-Analysis. J Cancer. 2016;7(9):1105–13.
Hench IB, Hench J, Tolnay M. Liquid Biopsy in Clinical Management of Breast, Lung, and Colorectal Cancer. Front Med (Lausanne). 2018;5:9. doi: 10.3389/ fmed.2018.00009.
O’Leary B, Hrebien S, Morden JP, Beaney M, Fribbens C, Huang X, et al. Early circulating tumor DNA dynamics and clonal selection with palbociclib and fulvestrant for breast cancer. Nat Commun. 2018;9(1):896. doi: 10.1038/s41467-018-03215-x.
Yadav DK, Bai X, Yadav RK, Singh A, Li G, Ma T, et al. Liquid biopsy in pancreatic cancer: the beginning of a new era. Oncotarget. 2018;9(42):26900–33.
Shapiro B, Chakrabarty M, Cohn EM, Leon SA. Determination of circulating DNA levels in patients with benign or malignant gastrointestinal disease. Cancer. 1983;51(11):2116–20.
Tabernero J, Lenz H-J, Siena S, Sobrero A, Falcone A, Ychou M, et al. Analysis of circulating DNA and protein biomarkers to predict the clinical activity of regorafenib and assess prognosis in patients with metastatic colorectal cancer: a retrospective, exploratory analysis of the CORRECT trial. Lancet Oncol. 2015;16(8):937–48.
Tjensvoll K, Lapin M, Buhl T, Oltedal S, Steen-Ottosen Berry K, Gilje B, et al. Clinical relevance of circulating KRAS mutated DNA in plasma from patients with advanced pancreatic cancer. Mol Oncol. 2016;10(4):635–43.
Cohen PA, Flowers N, Tong S, Hannan N, Pertile MD, Hui L. Abnormal plasma DNA profiles in early ovarian cancer using a non-invasive prenatal testing platform: implications for cancer screening. BMC Med. 2016;14(1):126.
Okajima W, Komatsu S, Ichikawa D, Miyamae M, Ohashi T, Imamura T, et al. Liquid biopsy in patients with hepatocellular carcinoma: Circulating tumor cells and cell-free nucleic acids. World J Gastroenterol. 2017;23(31):5650–68.
Payne K, Spruce R, Beggs A, Sharma N, Kong A, Martin T, et al. Circulating tumor DNA as a biomarker and liquid biopsy in head and neck squamous cell carcinoma. Head Neck. 2018;40(7):1598–604.
Bertero L, Siravegna G, Rudà R, Soffietti R, Bardelli A, Cassoni P. Review: Peering through a keyhole: liquid biopsy in primary and metastatic central nervous system tumours. Neuropathol Appl Neurobiol. 2019;45(7):655-670. doi: 10.1111/nan.12553.
Boire A, Brandsma D, Brastianos PK, Le Rhun E, Ahluwalia M, Junck L, et al. Liquid biopsy in central nervous system metastases: a RANO review and proposals for clinical applications. Neuro-oncology. 2019;21(5):571–84.