EDITORIAL
Liliana Gutiérrez¹, Briegel de las Salas¹, Natalia Sánchez¹, Luis Raez², Oscar Arrieta³, Andrés F. Cardona¹
Institute for Research, Science and Education, Luis Carlos Sarmiento Angulo Cancer Treatment and Research Center (CTIC), Bogotá, Colombia
Thoracic Oncology Program and Research Director of Memorial Health Care System (MHS), Miami, FL, US
Thoracic Oncology Unit, Instituto Nacional de Cancerología – INCaN, México City, México
Recibido:
1 de noviembre, 2023
Aceptado:
15 de noviembre, 2023
Correspondencia:
DOI: 10.56050/01205498.2305
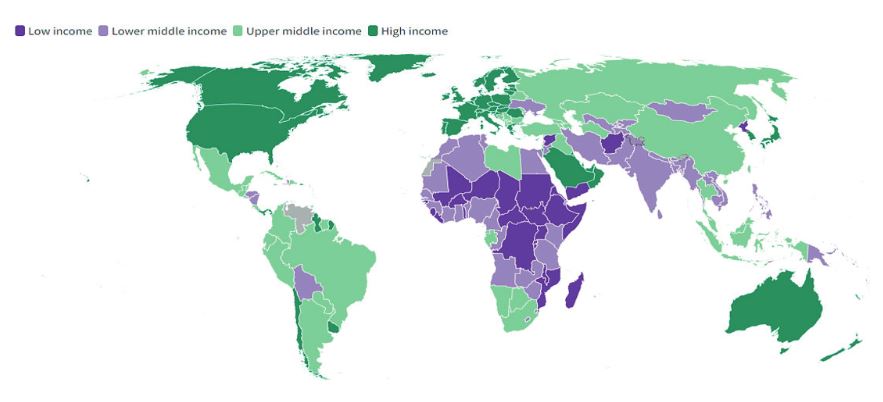
The World Bank classifies economies for analytical purposes into four income groups: low, lower-middle, upper-middle, and high-income. For this purpose, it uses gross national income (GNI) per capita data in U.S. dollars, converted from local currency using the World Bank Atlas (Figure 1), which is applied to smooth exchange rate fluctuations (1). Noncommunicable diseases (NCDs) were identified as one major challenge to sustainable development in low- and middle-income countries (LMICs). Most deaths globally are now due to NCDs, with cancer being responsible for at least 20 % of all mortality (2). Although the overall incidence of cancer is lower in LMICs compared with high-income countries (HICs), total cancer-related mortality is significantly higher in LMICs, especially for people ≤65 years of age; the more significant economic impact because of premature mortality and lost years of productivity is a particular problem for these limited resources environments (3). In 2020, 75 % of all global deaths attributable to NCDs, including cancer, occurred in LMICs, with nearly 50 % of deaths considered to be premature (4,5).
Worldwide, an estimated 19.3 million new cancer cases (18.1 million excluding nonmelanoma skin cancer) and almost 10.0 million cancer deaths occurred in 2020 (6). Breast cancer is the most diagnosed cancer, with an estimated 2.3 million new cases (11.7 %), followed by lung (11.4 %), colorectal (10.0 %), prostate (7.3 %), and stomach (5.6 %) neoplasms. Additionally, Lung cancer remained the leading cause of cancer death, with an estimated 1.8 million deaths (18 %), followed by colorectal (9.4 %), liver (8.3 %), stomach (7.7 %), and female breast (6.9 %) cancers.
Figure 1. The world by income and region (The World Bank Atlas, 2022). Countries are classified each year on July 1, the start of the World Bank fiscal year, based on GNI per capita data (https://datatopics.worldbank.org/ world-development-indicators/the-world-by-income-and-region.html).
Overall incidence was from 2-fold to 3-fold higher in transitioned versus transitioning countries for both sexes, whereas mortality varied <2-fold for men and little for women (6). By 2030, 75 % of all cancer deaths globally will occur in LMICs due to limited risk factor control (infection-associated cancers and absence of other preventive measures), educational resources, screening and surveillance programs, and scarce access to cancer therapies. On the other hand, LMICs have been experiencing increasing cancer-related mortality because of rising obesity rates, increasingly sedentary lifestyles, dietary factors, excess tobacco and alcohol use, and persistent carcinogenic infections like Helicobacter pylori, hepatitis B virus, and human papillomavirus (HPV) (7). Of the 16 million new cancer diagnoses globally in 2015, 16 % overall were attributable to these infectious agents. Indeed, the population-attributable percentage was significantly higher in less-developed countries than in developed ones, with some countries in sub-Saharan Africa having greater than 50 % attributable fractions related to infectious agents versus less than 5 % in the United States and Canada (7,8). Especially striking is that up to one-third of infection-attributable cancers arise in people younger than age 50 years, which partially accounts for the excessive premature deaths because of cancer in LMICs and further highlights the economic burden (8).
Efforts for cancer control in LMICs should aim to reduce exposure to common modifiable risk factors, improve access to care, and improve clinical outcomes (9). While ongoing efforts focus predominantly on expanding and strengthening treatment facilities, relatively less attention is paid to generating country-specific evidence for effective prevention, early detection, access, survivorship, and palliation, emphasizing quality and value (10). Cancer research is heavily skewed toward HICs, with disproportionately less research conducted in LMICs (11). For example, of all phase 3 trials of anti-cancer therapies conducted worldwide between 2014 and 2017, only 8 % were initiated and developed in LMICs, despite increasing recognition that trial results are not necessarily generalizable across populations (11). In addition, less than 1.3 % of the information on the molecular characteristics of solid and hematological tumors comes from research in LMICs (12). This problem is especially evident in South Asia, Africa, and Latin America. In Latin America, the main challenges to participation in clinical trials and institutional cancer research are the lack of public and private investment, scarcity of local funding, and delays in research regulatory processes (13).
The low level of investment in cancer research is a significant barrier to local and regional initiatives investigating tailored strategies among the Hispanic population. The percentage of gross domestic product (GDP) spent on research and development during 2008–2015 in Latin American countries was 0.66 %, varying from 1.18 in Brazil, 0.6 in Argentina, 0.4 in Mexico, 0.37 in Chile, 0.15 in Colombia, and 0.15 in Peru. This is 3.4 times less than in developed countries, such as South Korea, Japan, the US, and Germany, with GDP rates of 3.74, 3.36, 2.9, and 2.8, respectively (14,15). The limited number of cancer specialists and the lack of formal training in research procedures can cripple participation in cancer research. Matthew et al. reported that the ratio of clinical oncologists per new cancer diagnosis in high-middle-income Latin American countries ranges from 1:170 in Brazil, 1:287 in Argentina, 1:331 in Peru, to 1:667 in Chile, which compares unfavorably to the ratio of 1:137 found in the United States (16). In addition, most governmental grants available in Latin America and the Caribbean are insufficient to maintain competitive research endeavors (17). Notably, 6.1 % of medical oncologists from Latin America and the Caribbean declared they were the main sponsors of their research proposals in 2009–2010, with up to 41.2 % Mexican and 25 % Peruvian physicians stating that they supported their projects with their resources (18). Despite all the notable limitations that cancer research has in Latin America, a steady rise in scientific publications in oncology has been observed in recent years (19,20). Brazil was the most prolific country in 2020, with 1561 citable documents (45.8 %), followed by Mexico (19.8 %) and Argentina (7.9 %). However, despite recent advances, the scientific productivity of the region still needs to catch up to Northern America (33,710 citable documents published in 2020) and Western Europe (44,416 papers) (20).
Several gaps in cancer research of LMICs, including Latin America, need to be addressed to promote relevant results and innovation. These include the need for more reliable data, a scarcity of clinical trials, and a lack of an environment conducive to research in academic institutions, including infrastructure, trained human resources, protected time, and funding (10). National and institutional cancer data are required to assess the magnitude of cancer burden and an essential point to evaluate the efficacy or otherwise of any intervention in clinical care. Site-specific cancer incidence, mortality, and stage are poorly characterized or absent in many LMICs, with only one in five countries able to report data of sufficient quality to determine minimal estimates (10). For example, the coverage with population-based cancer registries (PBCRs) remains low in Latin America (a registry covers 19 % of the total population), Asia (15 %), and Africa (13 %), and sampling is predominantly sub-national, urban biased and of variable quality (21). A representative study found that, among 190 countries, 50 (26 %) did not have any cancer registry, 99 (52 %) had PBCRs, and only 81 (43 %) had national coverage (22). While 88 % of HICs and 49 % of upper-middle-income countries had PBCRs, only 32 % of LMICs and 24 % of low-income countries had PBCR data; national coverage of registries was 70 %, 44 %, 26 %, and 17 % in HICs, upper middle-income, lower middle-income, and low-income countries, respectively (22). Creating reliable data sources such as nationally representative PB- CRs should be prioritized by all countries to guide their cancer-control plans and research priorities.
Over 40 years, most HICs have developed excellent research capacity and infrastructure with trained and experienced researchers, clinical trial units (CTUs), research managers, and biostatistical support. In contrast, clinicians and researchers in LMICs lack formal training in research methods and are ill-equipped to conduct clinical and translational cancer research. Therefore, enhancing knowledge and skills is a crucial element of strengthening global research capacity—however, programs designed to accomplish this need to be adapted to the local context. For example, many LMICs have a limited number of health professionals treating cancer, and programs requiring 1 or 2 dedicated years of training in a different organization may not be feasible. Shorter-duration courses on clinical research methodology and protocol-development workshops offer early-career researcher’s opportunities to learn research methods (23). Nevertheless, continued mentoring from experienced investigators in their institutions supported by online virtual mentoring by external experts could give early-career researchers the skills to conduct independent research. However, future longer-term emphasis should be on formal research training, which provides a deeper and more thorough understanding of research methods.
Many LMICs must prioritize research sufficiently to establish adequate infrastructure for institutional researchers. Creating CTUs, academic contract research organizations, and institutional ethics committees or review boards facilitates research by supporting study design, biostatistics, data management, regulatory submissions, approvals, contracts, and trial insurance. The critical components of a comprehensive CTU include clinicians with broad experience in conducting clinical trials, biostatisticians, trial- and study-management teams (clinical research coordinators, study monitors, clinical project managers, and data managers), database-management systems, and administrative staff. A robust ethics and regulatory framework are crucial to ensure good clinical research practices and high-quality research conduct; establishing this well before starting research is essential. Organizational support should also include curating core facilities, datasets, biobanks, and other resources that benefit multiple investigators, particularly those at early-career stages. Another opportunity to improve the quality of research is participation in pharma-sponsored studies (24).
Collaborations and networks are crucial to promoting research in LMICs. Most partnerships in LMICs have been with HICs, resulting in unequal involvement and return in the short and long term (24). Furthermore, LMIC researchers are merely research implementers with marginal participation in its design and management (25). Various fronts have identified some essential criteria to favor mutual collaboration and the development derived from it, among others, the determination of opportunities for active involvement in cutting-edge research, exciting science, effective leadership, the competence of potential partners in, and commitment to good scientific practice, capacity building, respect for the needs, interests, and agendas of partners, open opportunities for discussion and disagreement, and generate trust and confidence in open collaboration (25). In the same way, governments, national research organizations, and funding bodies should work in concert to promote a ‘culture’ of research and integrate science and technology strategy at a political level. Fostering leadership in research, providing incentives for high-quality research, and adequate funding opportunities are necessary to motivate researchers in LMICs (25). Figure 2 includes the authorship network for cancer research in LATAM by country and the primary regional needs to expand cancer research.
In conclusion, it is essential to highlight some critical points for cancer research in LMICs, including those in Latin America. First, there is a reduction in the burden of patients diagnosed with advanced-stage cancers because nearly 75 % of cases in regions with less economic access are diagnosed in advanced stages, including neoplasms that are amenable to early diagnosis using various screening methods. Second, generate research on improving access to and affordability and outcomes of cancer care due to barriers to access, high cost, and lower quality of care.
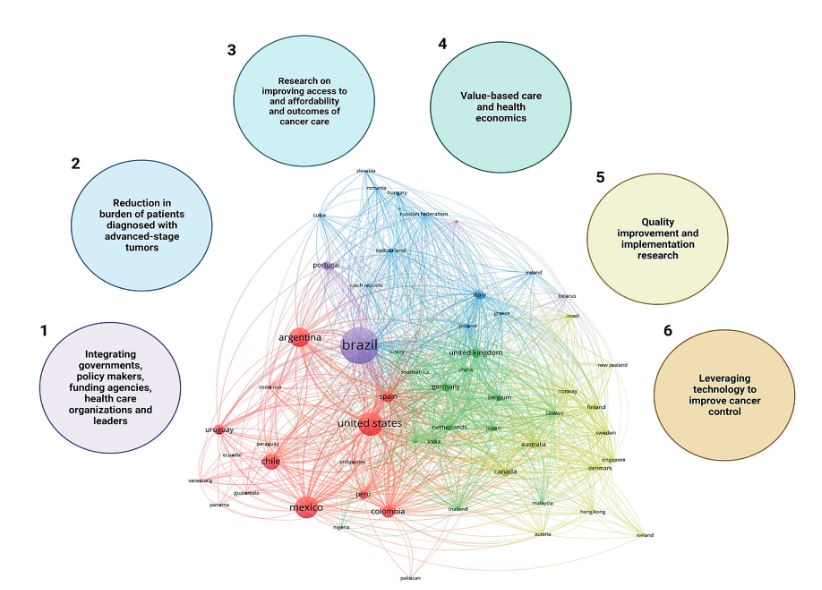
Figure 2. Authorship network for cancer research in LATAM by country and the principal needs to expand cancer research regionally.
Third, favor the development of value-based care and health economics research, considering that only 8–14 % of published economic evaluations of health interventions are from LMICs (27). Fourth, implement quality improvement and implementation research using real-life data and evidence. In the US and Europe, 30–50 % of patients do not receive optimal evidence-based clinical interventions, which is likely much higher in LMICs. Implementation gaps are a significant cause of the failure of health policies and reforms, such as decentralization of care delivery, healthcare regulation, and improvement of primary health care in LMICs (28). And finally, leveraging technology to improve cancer control.
Global cancer research has thus far been driven primarily by HICs, which have different cancer statistics, research priorities, capacity, infrastructure, and health systems than LMICs. Adopting research generated by HICs is likely to yield suboptimal outcomes for LMICs, and there is a need to urgently scale up locally relevant cancer research in these underrepresented countries. Strengthening research capacity at individual, organizational, network, and policy levels is vital for long-term benefit and sustainability. LMICs have an excellent opportunity to address important questions in cancer research that could impact cancer control globally. Governments, policymakers, funding agencies, healthcare organizations, leaders, researchers, and the public should cooperate and firmly commit to promoting cancer research in LMICs.
The World Bank. [Internet]. [Consultado marzo 3 de 2023]. Disponible en: https://datatopics.worldbank.org/world-development-indicators/the-world-by-income-and-region.html
WHO NCD mortality and morbidity. [Internet]. [Consultado marzo 3 de 2023]. Disponible en: https://www.who.int/gho/ncd/mortality_morbidity/en
Shah SC, Kayamba V, Peek RM Jr, Heimburger D. Cancer Control in Lowand Middle-Income Countries: Is It Time to Consider Screening? J Glob Oncol. 2019;5:1-8. doi: 10.1200/JGO.18.00200.
WHO The top 10 causes of death. [Internet]. [Consultado marzo 3 de 2023]. Disponible en: http://www.who.int/mediacentre/factsheets/fs310/en/index1.html
Sankaranarayanan R. Screening for cancer in low- and middle-income countries. Ann Glob Health. 2014;80:412-417.
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209-249. doi: 10.3322/caac.21660.
Ansari KK, Jha A. Causes of Cancer in the World: Comparative Risk Assessment of Nine Behavioral and Environmental Risk Factors. Cureus. 2022;14(9):e28875. doi: 10.7759/cureus.28875.
Schottenfeld D, Beebe-Dimmer J. The cancer burden attributable to biologic agents. Ann Epidemiol. 2015;25(3):183-7. doi: 10.1016/j.annepidem.2014.11.016.
Gelband H, Sankaranarayanan R, Gauvreau CL, Horton S, Anderson BO, Bray F, et al.; Disease Control Priorities-3 Cancer Author Group. Costs, affordability, and feasibility of an essential package of cancer control interventions in low-income and middle-income countries: key messages from Disease Control Priorities, 3rd edition. Lancet. 2016;387(10033):2133-2144. doi: 10.1016/S0140- 6736(15)00755-2.
Pramesh CS, Badwe RA, Bhoo-Pathy N, Booth CM, Chinnaswamy G, Dare AJ, et al. Priorities for cancer research in low- and middle-income countries: a global perspective. Nat Med. 2022;28(4):649-657. doi: 10.1038/s41591-022-01738-x.
Wells JC, Sharma S, Del Paggio JC, Hopman WM, Gyawali B, Mukherji D, et al. An Analysis of Contemporary Oncology Randomized Clinical Trials From Low/Middle-Income vs High-Income Countries. JAMA Oncol. 2021;7(3):379-385. doi: 10.1001/jamaoncol.2020.7478.
Drake TM, Knight SR, Harrison EM, Søreide K. Global Inequities in Precision Medicine and Molecular Cancer Research. Front Oncol. 2018;8:346. doi: 10.3389/fonc.2018.00346.
Gössling G, Rebelatto TF, Villarreal-Garza C, Ferrigno AS, Bretel D, Sala R, et al. Current Scenario of Clinical Cancer Research in Latin America and the Caribbean. Curr Oncol. 2023;30(1):653-662. doi: 10.3390/curroncol30010050.
UNESCO Institute for Statistics . Research and Development Expenditure (% of GDP)—Latin America & Caribbean. UNESCO Institute for Statistics; Montreal, QC, Canada: 2021.
Access to cancer medicine in low-resource settings. Lancet Oncol. 2013;14(1):1. doi: 10.1016/S1470- 2045(12)70595-8.
Mathew A. Global Survey of Clinical Oncology Workforce. J Glob Oncol. 2018;4:1-12. doi: 10.1200/ JGO.17.00188.
Ciocca DR, Delgado G. The reality of scientific research in Latin America; an insider’s perspective. Cell Stress Chaperones. 2017;22(6):847-852. doi: 10.1007/s12192-017-0815-8.
Gómez HL, Pinto JA, Castañeda C, Vallejos CS. Current barriers for developing clinical research in Latin America: A cross-sectional survey of medical oncologists. Clin. Res. Trials. 2015;1:22–28. doi: 10.15761/ CRT.1000108.
da Silva RE, Amato AA, Guilhem DB, de Carvalho MR, Novaes MRCG. International Clinical Trials in Latin American and Caribbean Countries: Research and Development to Meet Local Health Needs. Front Pharmacol. 2018;8:961. doi: 10.3389/ fphar.2017.00961.
Ruiz-Patiño A, Cardona AF, Arrieta O, Rolfo C, Gómez HL, Raez LE, et al. Scientific publications in cancer: in Latin America, strong scientific networks increase productivity (the TENJIN study). J Clin Epidemiol. 2020;126:1-8. doi: 10.1016/j.jclinepi.2020.05.033.
Bray F, Ferlay J, Laversanne M, Brewster DH, Gombe Mbalawa C, Kohler B, et al. Cancer Incidence in Five Continents: Inclusion criteria, highlights from Volume X and the global status of cancer registration. Int J Cancer. 2015;137(9):2060-71. doi: 10.1002/ ijc.29670.
Siddiqui AH, Zafar SN. Global Availability of Cancer Registry Data. J Glob Oncol. 2018;4:1-3. doi: 10.1200/JGO.18.00116.
Ranganathan P, Chinnaswamy G, Sengar M, Gadgil D, Thiagarajan S, Bhargava B, et al.; National Cancer Grid of India. The International Collaboration for Research methods Development in Oncology (CRe- DO) workshops: shaping the future of global oncology research. Lancet Oncol. 2021;22(8):e369-e376. doi: 10.1016/S1470-2045(21)00077-2.
Malekzadeh A, Michels K, Wolfman C, Anand N, Sturke R. Strengthening research capacity in LMICs to address the global NCD burden. Glob Health Action. 2020;13(1):1846904. doi: 10.1080/16549716.2020.1846904.
Munung NS, Mayosi BM, de Vries J. Equity in international health research collaborations in Africa: Perceptions and expectations of African researchers. PLoS One. 2017;12(10):e0186237. doi: 10.1371/ journal.pone.0186237.
Parker M, Kingori P. Good and Bad Research Collaborations: Researchers’ Views on Science and Ethics in Global Health Research. PLoS One. 2016 Oct 13;11(10):e0163579. doi: 10.1371/journal. pone.0163579.
Pitt C, Goodman C, Hanson K. Economic Evaluation in Global Perspective: A Bibliometric Analysis of the Recent Literature. Health Econ. 2016;25 Suppl 1(Suppl Suppl 1):9-28. doi: 10.1002/hec.3305.
Grol R. Successes and failures in the implementation of evidence-based guidelines for clinical practice. Med Care. 2001;39(8 Suppl 2):II46-54. doi: 10.1097/00005650-200108002-00003.